

PLAGUE JOURNAL February 2021: What Can We Learn from Africa (again), Part 1
PLAGUE JOURNAL February 2021: What Can We Learn from Africa (again), Part 1
Head-scratching about Africa reveals how badly the media get things wrong.

[Note: All Plague Journal entries were written as events unfolded. I have edited the drafts for clarity, but the tone and content are original, reflecting what we could see at the time.]
[This is the first of a two-part story. Part 2 can be found here.]
Last May (2020), after I’d spent the better part of two days and nights looking up temperatures and climate around the world, I got one of the best laughs of our pandemic when I saw this New Yorker headline: “What African Nations are Teaching the West about Fighting the Coronavirus.” The article was by Jina Moore. I didn’t read it. The title perfectly captured the blindness of the press to all things corona.
I still haven’t read it nine months later, but we can make some assumptions about its contents from where it fell along the corona timeline. March brought us panic, lockdowns, and the zombie metaphor (get within six feet of someone and you’re done). April was all race, gender, and essential workers, even if grocery workers and truck drivers remained healthier and saner than many wealthy people who hid in their homes. By May, as cases and fatality rates dropped, the stories were all about strong female leaders who crushed the virus, and about unity, trust, equality. The press, perhaps fearing they were losing the story, began to demand masks on everyone. By June, when fatalities were at their lowest, the headlines were full of bleak warnings about surging and spiking in Texas and Arizona and Florida. Early July was the heyday of the populist-strongmen narrative, people who downplayed the virus. (Apparently this virus could smell a punk.)
The timing of the original New Yorker article about Africa, published on May 14th, 2020, placed it squarely in the era of unity and female virtue—but Moore would have had trouble finding many female leaders or feel-good stories about healthcare in Africa, so we can guess that she may have pursued the vague (yet popular) thesis of grass-roots action, strong community, vigilance, and stoicism in the face of suffering. She may have included something about wisdom gained from experience with SARs and Ebola. The genre concedes a few problems at the governmental level but celebrates virtue in the population. We usually learn the names of a few strong women who have worked tirelessly for decades to bring clean water or other humble improvements to impoverished areas. We are likely to see a photograph of people standing outside a makeshift medical center, photogenic in their suffering.
The stories are fact-free, but we like them, so they keep coming. Now, at the end of 2020, ten months into our pandemic, we had no news, no reporting, no research. The press sold only fear and anger. The medical journals and institutions were full of researchers chasing professional citations and links from the Times. There were pages to fill, so the same stories were written and re-written as if by bots.
When a new article promising to explain Africa’s success landed in my inbox in December, I couldn’t resist. We knew by now that any coronavirus story would be about masks, distancing, and hand-washing. Given the absurdity of such claims across an entire continent, we could guess there would be some vague metaphysics about attitude, grace, unity, effort. We knew that any story about Africa would be patronizing.
The article arrived, as most do, uninvited through my screen, in an email from online question-and-answer platform Quora. The email asked the question, “Why/how is Africa more resistant to Covid?” Then this teaser: “‘Most African countries don’t have a peak. I don’t understand why. I’m completely at sea,’ admitted Professor Salim Karim - a le . . .”
I followed the link and landed on a BBC article from October 7th (2020) called “Coronavirus in Africa: Five reasons why Covid-19 has been less deadly than elsewhere.” The article begins with the scoresheet: “Africa has recorded about 37,000 deaths, compared with roughly 580,000 in the Americas, 230,000 in Europe, and 205,000 in Asia.” We learn that the case fatality rate is lower in Africa than globally. “So what are some of the reasons for Africa’s relatively low death rate?”
Here are the five reasons Africa beat the coronavirus, according to the BBC:
Reason 1: “Quick action”

The first thing we see is a photograph of a man under a plexiglass face shield worshipping in a church. Is this the kind of quick action we should all be taking? It would be tough in the U.S., where churches remain closed across much of the country.
We learn that Egypt’s first case was identified on February 14th. “So, right from the beginning, most African governments took drastic measures to try and slow the spread of the virus. Public health measures—including avoiding handshakes, frequent hand-washing, social distancing and wearing of face masks—were swiftly introduced.”
So that’s how they did it: with the same plan as every country on Earth. The BBC could have written the same throwaway line about any country anywhere—if the intent was to bestow praise—and it would tell us nothing about how citizens actually behaved. And Africa is a continent, not a country, so there would be wide variation in behavior and policy from one place to the next.
We know that masks were strongly discouraged by all major health institutions, including the WHO and the CDC, in February and March, so the BBC explanation is not only flimsy but false. A quick search for Africa photographs from March turns up a photo essay called “Africa’s week in pictures: 6-12 March 2020” from—of all places—the BBC. Promising “a selection of the week’s best photos from across the continent and beyond,” the gallery includes 22 colorful and arresting images. We see hundreds of people, mostly in groups, across various activities, but we see virtually no masks, at least the kind the BBC implies. We see many people in close proximity wearing traditional African masks, but not corona masks. We get one shot of a man wearing a cloth mask, in a photo specifically referencing the coronavirus. The only other nod to the coronavirus is a picture of a young girl washing her hands at a public basin in Kigali. Clearly, neither the citizens of these African countries nor the editors at the BBC gave much thought to the coronavirus or masks or distance or hand-washing or lockdowns when they gathered these photographs in early March.
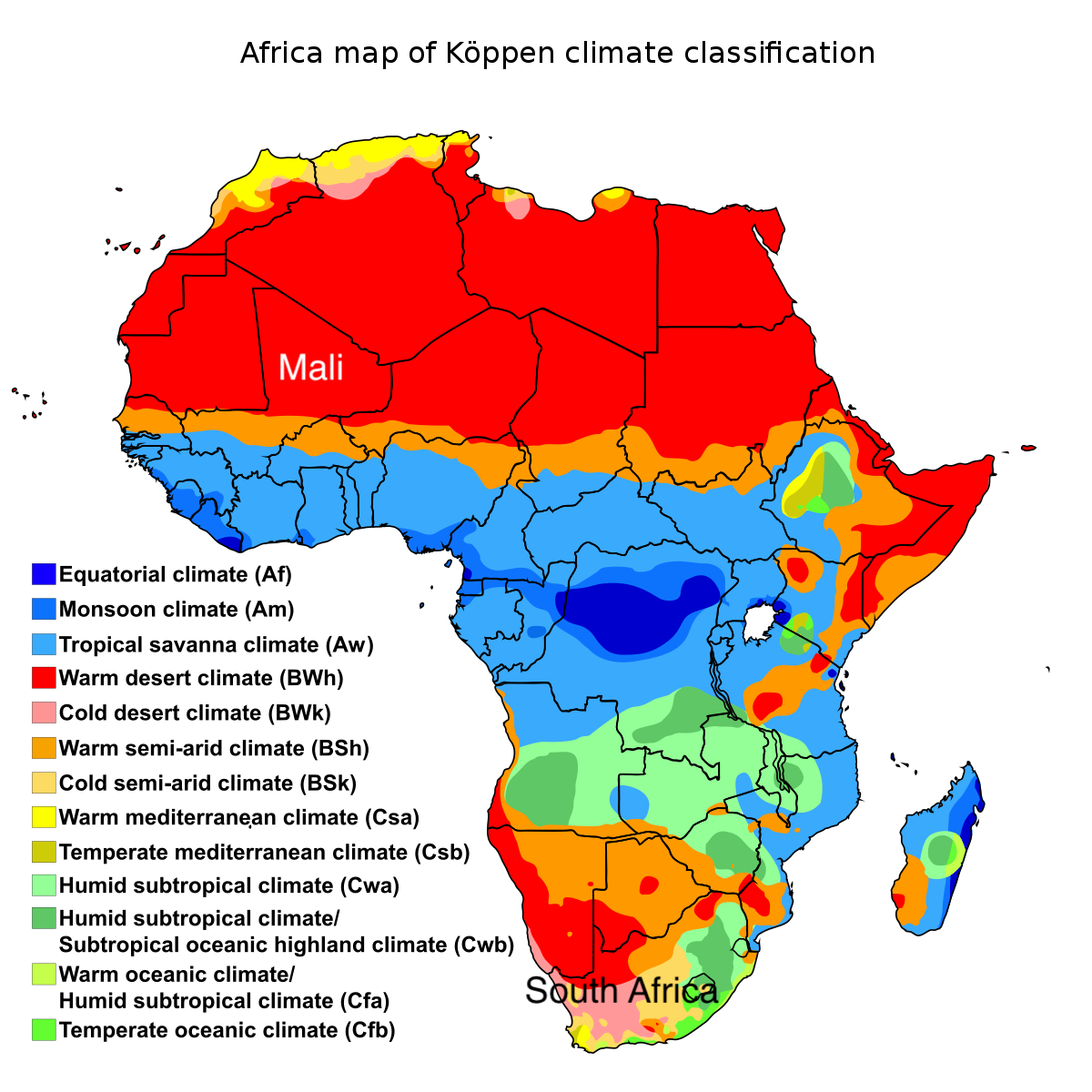
If African countries issued decrees in February, large segments of the population ignored them. And why not? There was virtually no risk from the virus. Africa was hot and humid or hot and dry. Even in the south, things were warm and clear in February and March. In an example of how governments have been getting things exactly backward with their corona policies, the BBC tells us that “only days after the lockdown was lifted—in early May—did Lesotho find its first confirmed cases. In a population of more than 2 million, it has so far recorded about 1,700 cases and 40 deaths.” Lesotho is a small enclave surrounded by South Africa at 30 degrees latitude, less than 100 miles from the South African coast. Beginning in May and June, Lesotho and much of neighboring South Africa experience temperate, cool weather—Koppen climate type Cfb. South Africa and Lesotho would experience the highest coronavirus rates in Africa after their winter low temperatures fell into the 30s. Lesotho locked down in March (summer), when the risk was low, and lifted its lockdown in May, when the risk was rapidly rising. The article implies that lifting the lockdown led to new cases, but the lockdowns were most likely irrelevant to the case rates.
Although the photos show people ignoring all of the safety practices credited in the article, viewed through a different lens we can see the actual reasons that coronavirus is not a threat in Africa, especially in March and April. We see mostly young people, who are outdoors in every photo. Even the vehicles lack roofs. It is a sunny climate, and people wear light clothing. They are young and thin, perhaps undernourished. There are few visible modern comforts.
Reason 2: “Public support”
Of course. Africans are so much better than we are. The BBC article says, “In a survey conducted in 18 countries in August by PERC, public support for safety measures was high—85% of respondents said they wore masks in the previous week.” The stories are always about masks. We could see in the March photos that people weren’t wearing masks—despite their “quick action.” What about August, when the survey took place? A desultory search turns up another BBC photo gallery: “Africa’s week in pictures: 14-20 August 2020.” We see more masks than in February, although many of them are around people’s necks. And one wonders about selection bias from the BBC. The August photos feature far fewer people, masked or otherwise, than the March photos did. Perhaps the BBC didn’t want us to notice how few masks there were in the general population?
We are not surprised to see masks on farmers in South Africa. We know that masks follow positive test counts, we know that South Africa has the highest case rates in Africa, and we know that their cases came during June, July, and August. Government orders and public opinion would naturally lead to widespread mask use as cases rapidly increased, as masks had spread across Europe and the U.S. following the initial peak in these places in April of 2020.
There is a photo of a crowd in Mali with raised fists and the caption, “President Ibrahim Boubacar Keita had been arrested earlier that day by Malian mutineers who stormed through the capital, Bamako.” The photo shows perhaps 35 or 40 people, and we can see about 20 faces but just one mask. What are the differences between South Africa and Mali that would cause different masking behavior?

The answer is the same one we find worldwide, which is risk: people wear masks when they are afraid. South Africa has 811 fatalities per million while Mali has just 17 per million (as of late February 2021). How can that be, when our news stories have told us all along that masks and distance and lockdowns provide our only protection? If politics and behavior cause all outcomes, Mali would have among the highest death rates in the world, judging from the photograph. But the stories are wrong. Corona outcomes are caused by weather, climate, and our exposure to nature—not by politics, masks, and proximity. People in countries with low wealth and few modern comforts are safer from coronavirus than people in wealthy countries with first-world diets and indoor heating and air-conditioning.

The claim of African “public support” is so vague as to be meaningless. These what-can-we-learn-from stories have to contain a certain number of items to make us click, so they make up a few things about masks and unity and hope we don’t look too closely. What does it mean to say that 85% “said they wore masks in the previous week”? Where did they wear them? How often? Even in countries with low mask-wearing, people would be expected or required to pull on a mask in certain places. In much of Europe and the U.S., roughly the same percentage of people—between 80% and 90%—reported that they “always” wore a mask, while the African survey asks only whether people “wore masks in the previous week.”
In another admission that undermines the article’s premise, we learn that “more and more countries have been forced to re-open their economies even though the number of cases is much higher than when they ordered the shutdowns.” If cases are “much higher” after lockdowns began, why do we continue to believe lockdowns are effective? And why would infections decline—which they did—after countries re-opened? The answer is that lockdowns are irrelevant: cases rise and fall, and they rise and fall most sharply in high latitudes in temperate climates.
3: “Young population - and few old-age homes”
Here we have the first true statement, sandwiched between layers of dogma. “Globally, most of those who have died have been aged over 80, while Africa is home to the world’s youngest population with a median age of 19 years, according to UN data.” The writer deserves credit for a rare bit of honesty: most who have died have been over 80. Average life expectancy is low in Africa, and it is true that if people die young, of malnutrition, AIDS, or malaria, they won’t be at risk of dying from COVID, which does not attack young people.
The WHO reports that “about 91% of Covid-19 infection in sub-Saharan Africa are among people below 60 years and over 80% are asymptomatic.” A young population living in the sun without indoor heating or air-conditioning, unburdened by a first-world diet, is largely immune from severe cases. Only three percent of Africa’s population is older than 65.
4: “Favourable climate”
Now they have landed on the essential truth—but they just scratch the edges of it, quoting a researcher from the University of Maryland who said his team had studied cities around the world and found that the virus “just spreads better when temperature and humidity drop.” The following sentence supports the theory: “African countries away from the Tropics have been worse off.” The researchers and the article miss that all of the hardest-hit places on Earth have been damp, cool, gray climates—including parts of South Africa and Lesotho in the winter. Although dry air fuels the spread of the virus, dry climates do not, for the simple reason that people spread it indoors. Cool damp outdoor air becomes warm dry indoor air when heated. The virus gets fortified in the lungs of people who breathe 35-degree outdoor air, then spreads in 70-degree dry indoor air.
Much of northern and eastern Africa has a dry climate, either desert or semi-arid, not tropical. According to the article, these regions should see a lot of spreading. But these arid regions of central Africa have neither cool outdoor air nor much heating or air-conditioning, or indoor living of any kind. South Africa along the coast is dangerous because the damp, cool winter air drives people inside—including many wealthy people, who can afford central heating. (And in the summer, these same people can afford air-conditioning, so there was a significant second wave in December and January, South Africa’s hottest months, similar to what we saw in Arizona, Texas, and Florida in June and July.) The increased coronavirus rates “away from the Tropics” in Africa are caused not by lower humidity but by temperate, cooler winter weather.
5: “Good community health systems”
The BBC’s final reason for Africa’s success is a throwaway: a feel-good ending to a satisfying story. The earlier reasons offered in the article are straight from the playbook: hand-washing, avoiding handshakes, distance, masks. Laughable, untrue, meaningless, but—quick action. Then we got “public support,” flimsy poll results telling us that people wore masks, long after the worldwide embrace of masks was reaching its peak although photographic evidence from Africa itself shows little masking. Then, perhaps to fill space, we got an unexpected bit of truth, about age and climate. We end with the vague homilies about “community health,” with nods to Africa’s history with Ebola and polio. We get no concrete information or data, just a few broad assertions and quotations, including from a Nigerian doctor, who said, “Once I heard the news, I instantly thought: duty is calling. My expertise is needed to serve my community.”
It was all just storytelling and propaganda. Africa has low coronavirus results for the same reasons that poor places around the world in hot climates have low coronavirus results: temperature, sun, low life expectancy, low obesity, and exposure to the elements.
[This is the first of a two-part story. Part 2 can be found here.]